Introduction
Background
In 1967, Tomisaku Kawasaki first described Kawasaki disease (KD) as a unique illness characterized by fever, rash, conjunctival injection, cervical lymphadenitis, inflammation of the lips and oral cavity, and erythema and edema of the hands and feet.1 Kawasaki disease is a generalized vasculitis of unknown etiology that has also been called mucocutaneous lymph node syndrome and infantile periarteritis nodosa. In developed countries, Kawasaki disease has replaced acute rheumatic fever as the most common cause of acquired heart disease in children.
Pathophysiology
The vasculitis is most severe in medium-sized arteries but can also occur in veins, capillaries, small arterioles, and larger arteries.
In severely affected vessels, the media develops inflammation with necrosis of smooth muscle cells. The internal and external elastic laminae can split, leading to aneurysms. Four to 8 weeks after the onset of symptoms, inflammatory changes are less apparent and fibrous connective tissue begins to form within the vessel wall. The intima proliferates and thickens. The vessel wall eventually becomes narrowed or occluded owing to stenosis or a thrombus. Cardiovascular death usually occurs from a myocardial infarction secondary to thrombosis of a coronary aneurysm or from rupture of a large coronary aneurysm.
The vasculitis also affects other medium-sized vessels, including the renal, paraovarian, paratesticular, mesenteric, pancreatic, iliac, hepatic, splenic, and axillary arteries, resulting in systemic aneurysms.
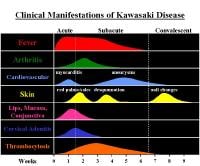
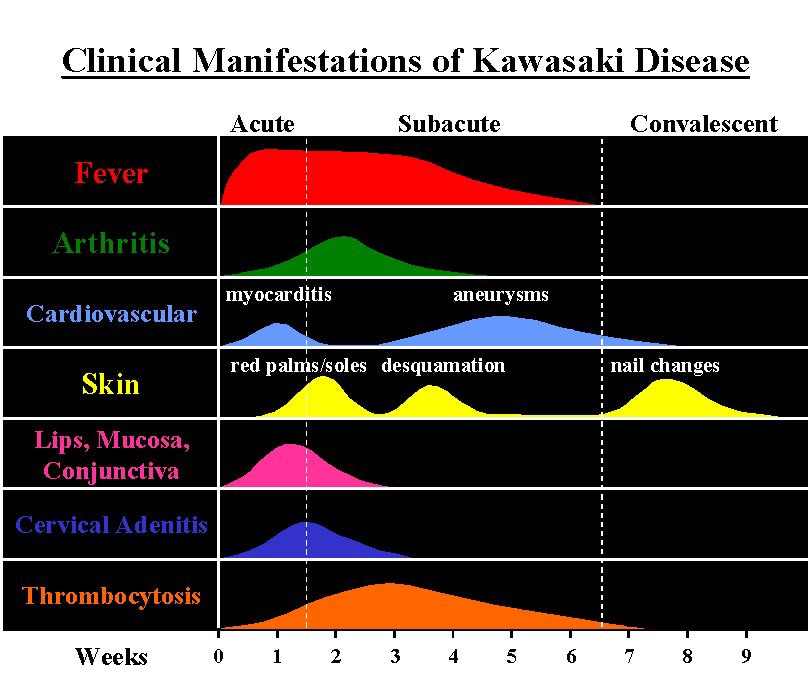
Clinical manifestations and time course of Kawasaki disease.
Frequency
United States
The mean annual incidence in children of non-Asian descent is 10 cases per 100,000 children younger than 5 years, and the mean annual incidence in children of Asian descent is 44 cases per 100,000 children younger than 5 years.
International
In Japan, the mean annual incidence is 95 cases per 100,000 children younger than 5 years.
Mortality/Morbidity
- Data are limited, but death occurs in approximately 1% of affected American children. In children younger than 1 year, the mortality rate may exceed 4%. In patients aged 1 year or older, the death rate is probably less than 1%.
- The average mortality rate in Japan is 0.1-0.3%.
- Coronary artery aneurysms develop in up to 25% of untreated patients. They develop in less than 5-10% of patients treated with intravenous gamma globulin before the 10th day of illness.
Race
The disease is more common in Asian children, especially those of Japanese descent.
Sex
- Disease occurs more often in males than in females (1.5:1).
- Death and serious complications are more common in males than females.
Age
- Most patients (ie, 80%) are affected when they are younger than 4 years; however, Kawasaki disease is rare in infants younger than 3 months. Kawasaki disease has been described in adolescents and adults.
- In the United States, the peak age of onset is 18-24 months.
- In Japan, the peak age of onset is 6-11 months.
Clinical
History
- Classic history of Kawasaki disease
- Fever
- Conjunctival injection
- Mucositis
- Changes in the peripheral extremities
- Erythematous rash
- Enlarged cervical lymph nodes
- Other symptoms
- Extreme irritability
- Joint pain or edema
- Poor oral intake
- Refusal to ambulate
- Refusal to hold objects
- Abdominal pain
- Nausea
- Diarrhea
Physical
Diagnosis is based on established clinical diagnostic criteria, including severe fevers for 5 days and 4 of the 5 other signs listed below. Kawasaki disease is a diagnosis of exclusion, so other diseases with similar findings (see Differentials) must first be ruled out. Patients with fever who appear to have Kawasaki disease but do not meet criteria and have no other cause of their illness are said to have atypical or incomplete Kawasaki disease. Patients with fever duration of at least 5 days and fewer than 4 of the principal criteria can be diagnosed with Kawasaki disease when coronary artery abnormalities are revealed by an echocardiogram or an angiogram. In the presence of 4 or more of the criteria, this condition can be diagnosed on day 4 of fever.
- Fever
- Fever, usually more than 39.9°C, for at least 5 days
- High spiking and remittent
- Persists 1-2 weeks without treatment
- May not respond to antipyretics
- Usually resolves in 1-2 days after treatment with intravenous gamma globulin
- Other signs
- Bilateral conjunctival injection without exudate
- Dry, erythematous, fissured lips that bleed easily
- Erythema of the oral and pharyngeal mucosa
- Strawberry tongue with prominent papillae and erythema

Oral manifestations of Kawasaki disease: red lips and strawberry tongue.
- No oral exudates, ulcerations, or Koplik spots
- Hands and feet
- Erythema of palms and soles, often with healthy skin on wrists and ankles
- Edema
- Periungual desquamation of fingers and toes about 2 weeks after onset
- Transverse grooves across the nails (Beau lines) 1-2 months after onset
- Erythematous rash
- Nonspecific, diffuse, maculopapular erythematous rash
- Possible scarlatiniform or erythema multiforme–type rash with target lesions
- Groin erythema or desquamation
- Fine pustules over extensor surfaces of extremities
- No observable vesicles or bullae
- Cervical lymphadenopathy
- Node diameter larger than 1.5 cm
- Observed in approximately 50-75% of patients
- Node - Sometimes erythematous but is not fluctuant or purulent and is not responsive to antibiotics
- Exclusion of other diseases with similar findings
- Miscellaneous
- Arthralgia and arthritis involving multiple joints (eg, including hands, knees, ankles, hips)
- Lethargy, headache, and stiff neck secondary to aseptic meningitis
- Meatitis, vulvitis, urethritis
- Signs of congestive heart failure (eg, S3 gallop, cardiomegaly, tachypnea, tachycardia from myocarditis)
- Otitis media
- Right-upper-quadrant abdominal mass or guarding secondary to gallbladder hydrops
- Jaundice
- Diarrhea
- Erythema and induration at the site of Bacille Calmette-Guérin (BCG) inoculation (common in Japan)
- Chest pain, abdominal pain, shock and/or emesis secondary to myocardial infarction in older children
- Cardiac murmur due to acute mitral insufficiency
- Severe peripheral ischemia with gangrene (rare)
- Diagnostic guidelines for Kawasaki disease include fever lasting more than 5 days, plus 4 of the following 5 criteria (other illnesses with similar clinical signs must be excluded):
- Polymorphous rash
- Bilateral conjunctival injection
- One or more of the following mucous membrane changes:
- Diffuse injection of oral and pharyngeal mucosa
- Erythema or fissuring of the lips
- Strawberry tongue
- Acute, nonpurulent cervical lymphadenopathy (one lymph node must be >1.5 cm)
- One or more of the following extremity changes:
- Erythema of palms and/or soles
- Indurative edema of hands and/or feet
- Membranous desquamation of the fingertips

Causes
Although the etiology of Kawasaki disease is unknown, the acute presentation and the clustering of cases suggest an infectious etiology. The production of various inflammatory cytokines, including interleukin-1 (IL-1), IL-6, tumor necrosis factor-alpha, and interferon gamma, is increased and may mediate vascular endothelial damage. Some cases of Kawasaki disease show familial susceptibility. Children in Japan who had had parents with Kawasaki disease seem to have a more severe form of this disease and are more susceptible to recurrence.2
Kawasaki disease likely has a genetic susceptibility. A genome-wide linkage analysis of affected sibling pairs was performed in Japan, and a multipoint linkage analysis identified evidence of linkage on chromosome 12q24.3

I was diagnose with genital warts since 2012 i have be taking lot treatment and all i got is outbreak. in 2015 I gave up the treatment because I can't continues wasting time and money on treatment at the end it will not cure me. about 6 weeks ago i did natural research online I had So many people talking good about natural remedy, after the research i was recommended to Dr onokun, And I wrote to him through his email and told him my problem after some conversations with him he gave me natural treatment after 1 week Dr onokun treated me i got cured permanently. and i went to see my doc he confirmed that the diseases has gone out from my body. every patients should know there is 100% natural hpv cure. contact Dr onokun his email address: dronokunherbalcure@gmail.com
Trả lờiXóa