Introduction
Multiple radiolucent or mixed radiolucent/radiopaque lesions of the mandible may present as incidental findings on radiographs or as the chief symptom of a patient. This article is not intended to be an all-inclusive discussion of such lesions; instead, it confines itself to an overview of the major odontogenic cysts and tumors with a brief discussion of other mandibular lesions that are often called cysts but are not true cystic lesions.
Although often similar in radiographic presentation, malignant tumors (both primary and metastatic), benign salivary tumors, and vascular lesions are not addressed herein. However, such lesions should be included in the differential diagnoses of a patient presenting with mandibular radiolucency or swelling. As a corollary, before the biopsy of any such lesions, the area should be aspirated to exclude a vascular lesion.
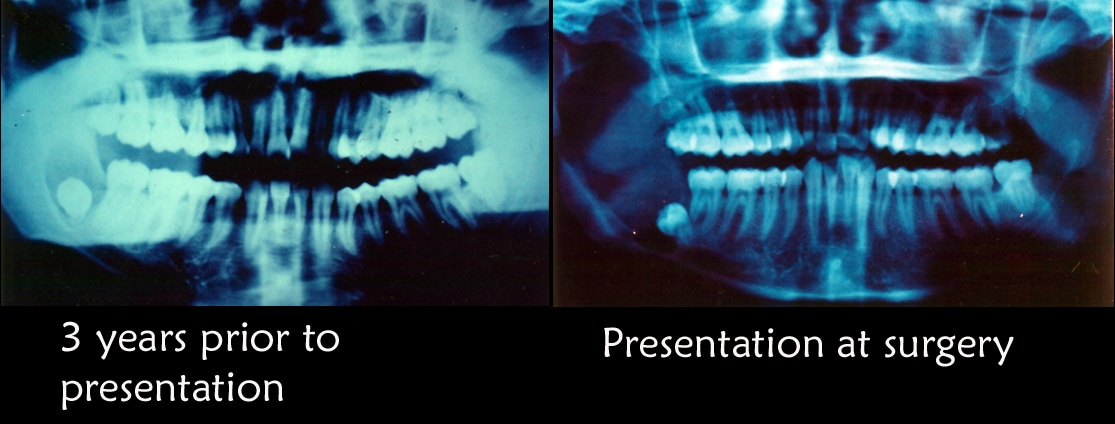
Initial radiographic appearance. The patient was advised that biopsy of cystic lesion was indicated; however, he did not schedule an appointment because he was planning to leave the country. He did not follow up for 3 years. He returned to the United States and sought care from a general dentist when he noted some mild facial swelling and discomfort. He was referred to the oral and maxillofacial surgery (OMFS) clinic. The second radiograph depicts the appearance of the lesion at the second presentation.

Odontogenic Mandibular Cysts
Odontogenic cysts are defined as epithelial-lined structures derived from odontogenic epithelium. Most odontogenic cysts are defined more by their location than by any histologic characteristics. Accordingly, the surgeon must provide the pathologist with appropriate history and radiographs when submitting such specimens for examination.
Periapical cyst
A periapical (radicular) cyst is the most common odontogenic cyst. The usual etiology is a tooth that becomes infected, leading to necrosis of the pulp. Toxins exit the apex of the tooth, leading to periapical inflammation. This inflammation stimulates the Malassez epithelial rests, which are found in the periodontal ligament, resulting in the formation of a periapical granuloma that may be infected or sterile. Eventually, this epithelium undergoes necrosis caused by a lack of blood supply, and the granuloma becomes a cyst. The lesions are not usually clinically detectable when small but most often are discovered as incidental findings on radiographic survey.
Radiographically, distinguishing between a granuloma and a cyst is impossible, although some say that if the lesion is quite large it is more likely to be a cyst.1 They both present as radiolucent lesions in association with the apex of a nonvital tooth. Occasionally, these lesions can become quite large because they grow in response to pressure. However, granulomas and cysts are not neoplastic.
Microscopically, the epithelium is a nondescript stratified squamous epithelium without keratin formation. Inflammatory changes may be observed in the cyst wall, and these changes, in turn, may lead to epithelial changes (eg, ulceration, atrophy, hyperplasia). In particularly inflamed lesions, cholesterol slits and/or foamy macrophages may be apparent.
Several treatment options exist for such cysts. Many cysts resolve with endodontic therapy of the involved tooth. Those lesions should be monitored radiographically to ensure such resolution. Lesions that fail to resolve with such therapy should be surgically removed and histopathologically examined. Although these cysts arise from a mature resting epithelium and thus have a relatively low growth potential, a squamous cell carcinoma occasionally may arise de novo in a radicular cyst, thus the recommendation for histopathologic examination of all tissues removed.
Dentigerous cyst
The second most common odontogenic cyst is the dentigerous cyst, which develops within the normal dental follicle that surrounds an unerupted tooth. The dentigerous cyst is not thought to be neoplastic. It most frequently is found in areas where unerupted teeth are found: mandibular third molars, maxillary third molars, and maxillary canines, in decreasing order of frequency. These cysts can grow very large and can move teeth, but, more commonly, they are relatively small. Most dentigerous cysts are asymptomatic, and their discovery is usually an incidental finding on radiography.
The usual radiographic appearance is that of a well-demarcated radiolucent lesion attached at an acute angle to the cervical area of an unerupted tooth. The border of the lesion may be radiopaque. The radiographic differentiation between a dentigerous cyst and a normal dental follicle is based merely on size.
However, histologically, a distinction other than size is found. The dental follicle is normally lined by the reduced enamel epithelium (see Odontogenesis), while the dentigerous cyst is lined with a stratified squamous nonkeratinizing epithelium. Dystrophic calcification and clusters of mucous cells may be found within the cysts.
Dentigerous cysts develop from follicular epithelium, and follicular epithelium has greater potential for growth, differentiation, and degeneration than the epithelium from which radicular cysts arise. Occasionally, other more ominous lesions arise within the walls of the dentigerous cyst, including mucoepidermoid carcinoma arising from mucous cells within the cyst walls, ameloblastoma (see Odontogenic tumors; 17% of ameloblastomas arise within a dentigerous cyst), and squamous cell carcinoma. As previously mentioned, dentigerous cysts also can become quite large and can place the patient at risk for pathologic jaw fracture.
These findings comprise most of the medical rationale for removal of impacted third molars with pericoronal radiolucencies; however, impacted teeth with small pericoronal radiolucencies (suggesting the presence of normal dental follicle rather than dentigerous cyst) may also be monitored with serial radiographic examination. Any increase in the size of the lesion should prompt removal and histopathologic examination. Any lesion that appears larger than a normal dental follicle indicates removal and histopathologic examination.
Primordial cyst
By definition, the primordial cyst develops instead of a tooth. Presumably, the dental follicle forms and subsequently undergoes cystic degeneration without ever completing odontogenesis. This is the rarest odontogenic cyst, and lesions designated as primordial cysts may represent residual cysts. The histology of these lesions is a nondescript stratified squamous epithelium. A complete dental history is important to establish a diagnosis of primordial (versus residual) cyst, although such a diagnosis often has little clinical significance in terms of treatment planning and decision making.
Residual cyst
Residual cyst is a term of convenience because no teeth are left by which to identify the lesion. Most commonly, these are actually retained periapical cysts from teeth that have been removed. The histology is a nondescript stratified squamous epithelium.
Lateral periodontal cyst
The name lateral periodontal cyst is a misnomer. These cysts are not inflammatory, they do not arise from periodontitis, and they are not a phenomenon associated with lateral canals within the tooth structure. These cysts are always well demarcated, relatively small, and radiolucent (sometimes with a radiopaque roof). They are most commonly associated with the mandibular premolar area and are occasionally found in the maxillary anterior. They are usually not clinically apparent but, rather, are detected through radiographic examination. These cysts have a distinctive histology consisting of a thick fibrous noninflamed cyst wall, and the lining epithelium is made of thin cuboidal cells. This lining is incomplete and easily sloughs away with mural thickenings of clear cells at periodic intervals. These cysts develop from the postfunctional dental lamina, and no good explanation is known for the localization that is shown.
Gingival cyst of the newborn
Gingival cysts of newborns generally occur in multiples but occasionally occur as solitary nodules. They are located on the alveolar ridges of newborns or young infants. These structures originate from remnants of the dental lamina and are located in the corium below the surface epithelium. Occasionally, they may become large enough to be clinically noticeable as discrete white swellings on the ridges. They are generally asymptomatic and do not produce any discomfort for the infant.
Bohn nodules and Epstein pearls are 2 similar lesions with which gingival cysts sometimes may be confused; however, the location and etiology of these lesions are somewhat different. Epstein pearls are cystic keratin-filled nodules found along the midpalatine raphe and are thought to be derived from entrapped epithelial remnants along the line of fusion. Bohn nodules are keratin-filled cysts scattered all over the palate, but they are most apparent at the junction of the hard and soft palate. These are thought to be derived from palatal salivary gland structures.
Histologically, the gingival cyst of the newborn is a true cyst with a thin epithelial lining. The lumen is usually filled with keratin but may contain some inflammatory cells, dystrophic calcifications, and hyaline bodies, such as those often found in dentigerous cysts.
No treatment is required for these lesions, which usually disappear either by opening onto the surface mucosa or through disruption by erupting teeth. These cysts are most likely what older literature describes as predeciduous dentition.
Gingival cyst of the adult
Gingival cysts of the adult are found only in soft tissue in the lower premolar areas. These cysts present as tense, fluctuant, vesicular, or bullous lesions. Histologically, they look like lateral periodontal cysts, and they probably represent the same lesion when found in soft tissue.
Odontogenic keratocyst (keratocystic odontogenic tumor)
The odontogenic keratocyst (OKC) is the most important of the odontogenic cysts. This cyst may have any clinical appearance; it is a great mimic, and the diagnosis is a histologic one. These lesions are different from other cysts; they are aggressive and can be difficult to remove. OKCs can grow quite rapidly, and recurrences are frequent. This is the third most common odontogenic cyst and belongs in the differential diagnoses of any radiolucency of the jaws. Although 40% of OKCs appear in a dentigerous relationship, 9% of dentigerous cysts are OKCs when the histology is examined. These cysts also are found as part of the basal cell nevus syndrome, also known as Gorlin syndrome (see the next section, Basal cell nevus syndrome).
Histologically, these cysts are formed with a stratified squamous epithelium that produces orthokeratin (10%), parakeratin (83%), or both types of keratin (7%). The epithelial lining appears corrugated when viewed under a microscope. A well-polarized hyperchromatic basal layer is observed, and the cells remain basaloid almost to the surface. No rete ridges are present; therefore, the epithelium often sloughs from the connective tissue (94% of the time). The epithelium is thin, and mitotic activity is frequent; therefore, OKCs grow in a neoplastic fashion and not in response to internal pressure. The lumen frequently is filled with a foul-smelling cheeselike material that is not pus but rather collected degenerating keratin.
The lesions grow in a multilocular bosselated fashion with daughter cysts that extend into the surrounding bone. Because of this relationship, the tendency for recurrence is high, particularly if the original surgical treatment does not result in complete removal of the lesion. Enucleations with peripheral ostectomy and/or cryosurgery are the most common forms of treatment. Long-term (lifetime) follow-up radiography is imperative. If these lesions are left untreated, they can become quite large and locally destructive.
The variant of OKC that produces only orthokeratin acts somewhat differently than other OKCs. These almost always are found in a dentigerous association, usually around the mandibular third molar, and they are much less aggressive. They do not have a hyperchromatic basal layer; in fact, the basal layer is flattened. They are not associated with basal cell nevus syndrome.
Basal cell nevus syndromeThis symptom complex includes hypertelorism, midface hypoplasia, relative frontal bossing and prognathism, mental retardation, schizophrenia, multiple basal cell carcinomas, calcification of the falx cerebri, bifid ribs, palmar pitting (the pits later develop into basal cell carcinoma), and multiple OKCs. Multiple OKCs are diagnostic for basal cell nevus syndrome until proven otherwise. This is a hereditary disease with autosomal dominant inheritance and high penetration. Of patients with OKC, 5% have basal cell nevus syndrome. Early identification of these patients and their lesions is key to improving long-term survival and quality of life.

I was diagnose with genital warts since 2012 i have be taking lot treatment and all i got is outbreak. in 2015 I gave up the treatment because I can't continues wasting time and money on treatment at the end it will not cure me. about 6 weeks ago i did natural research online I had So many people talking good about natural remedy, after the research i was recommended to Dr onokun, And I wrote to him through his email and told him my problem after some conversations with him he gave me natural treatment after 1 week Dr onokun treated me i got cured permanently. and i went to see my doc he confirmed that the diseases has gone out from my body. every patients should know there is 100% natural hpv cure. contact Dr onokun his email address: dronokunherbalcure@gmail.com
Trả lờiXóa