Introduction
Tympanic membrane perforation (TMP) is a condition as old as the human species.
Problem
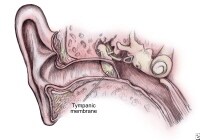
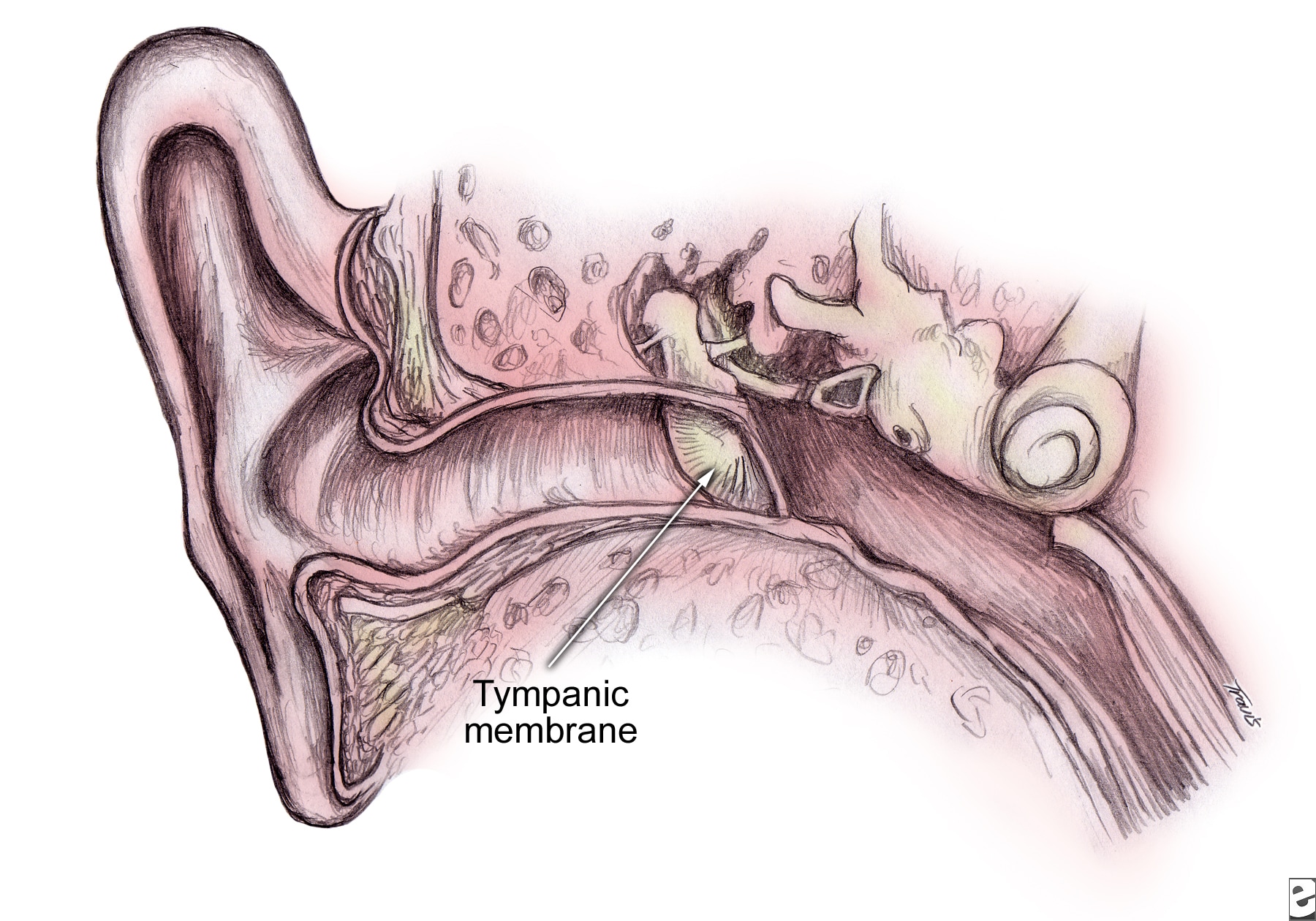
The tympanic membrane, also called the eardrum (or just the drum), is a stiff (but flexible), translucent, diaphragmlike structure. The eardrum moves synchronously in response to variations in air pressures, which constitute sound waves. The drum's vibrations are transmitted through the ossicular chain to the cochlea. In the cochlea, vibratory mechanical energy changes to electrochemical energy and streams via the eighth cranial nerve to the brain. The tympanic membrane and its attached ossicles thus act as a transducer, changing one form of energy into another form.
Tympanic membrane (TM) as continuation of the upper wall of external auditory canal (EAC) with angle of incline up to 45 degrees on the border between middle ear and the EAC.
Tympanic membrane perforations (TMPs) can result from disease (particularly infection), trauma, or medical care. Perforations can be temporary or persistent. Effect varies with size, location on the drum surface, and associated pathologic condition.
Frequency
Incidence of tympanic membrane perforation (TMP) in the general population is unknown. One survey found that that 4% of a population of Native American children had tympanic membrane perforation (TMP).1 Another study found that 3% of children treated with ventilation tubes had the condition.2 However, the incidence in the general population has not been studied. Even the exact number of surgical tympanic membrane perforation (TMP) repairs performed each year is unknown. Analysis of government statistics indicates that perhaps 150,000 tympanoplasties are performed per year in a population of 280 million.
Etiology
Infection is the principal cause of tympanic membrane perforation (TMP). Acute infection of the middle ear may cause a relative ischemia in the drum concurrent with increased pressure in the middle ear space. This leads to a tear or rupture of the eardrum that is usually preceded by severe pain. If the perforation does not heal, it leaves a residual tympanic membrane perforation (TMP).
A prominent school of thought now advocates less aggressive use of antibiotics. Those who hold this position recognize that many episodes of otitis media are caused by viruses, so they resolve spontaneously; advocates of this position desire to slow emergence of antibiotic-resistant bacterial strains. Evidence is emerging that an increased incidence of acute mastoiditis is resulting from reduced use of antibiotics.3 Time will tell whether increased incidence of perforation and other complications of otitis media, such as brain abscess, meningitis, and septic sigmoid sinus thrombosis, also occur.
Ear canal infections rarely cause tympanic membrane perforations (TMP). When this occurs, it is often associated with infection by Aspergillus niger.
Traumatic perforations may result from blows to the ear (eg, being struck with the flat of the hand; falling from water skis with the head hitting the water surface, ear down). Exposure to severe atmospheric overpressure from an explosion can tear the drum.4 Tympanic membrane perforation (TMP) from water pressure occurs in scuba divers, usually in a drum with atrophy from previous disease. Objects used to clean the ear canal can perforate the drum.
Inexpertly performed irrigation of the ear canal for wax can lead to perforation. In some settings, when irrigation for cerumen is relegated to medical assistants, otolaryngologists may see 10-20 patients per year with this injury. Evidence exists that such perforations are less likely to heal spontaneously.5 Tympanic membrane perforation (TMP) is intentionally created whenever a surgeon makes an incision in the eardrum (myringotomy). When pressure-equalizing tubes (ventilating tubes) are placed, the TMP purposely is held open. Failure of surgically created openings to heal when the tube extrudes results in chronic tympanic membrane perforation (TMP).
Pathophysiology
The eardrum tends to heal itself. Even eardrums that have been perforated multiple times often remain intact. At times, a perforation heals with a thin membrane consisting only of mucosal and squamous epithelial layers without a fibrous middle layer. Such a neomembrane may be so thin that it can be mistaken for a perforation instead of a healed perforation. Neomembranes may retract deeply into the middle ear, sometimes making them more difficult to distinguish from actual perforations. Examination under the operating microscope resolves ambiguity. Deep retraction, especially in the posterior superior quadrant of the drum, may presage formation of cholesteatoma.
The presence of perforation renders the ear more susceptible to infection if water enters the ear canal. If bacteria-contaminated water passes through the perforation, infection can result. Water surface tension may protect the ear from penetration through a very small perforation. This explains higher infection rates from hair washing than from swimming activities (ie, soap lowers surface tension so water can enter the middle ear). Presence of perforation is an absolute contraindication to irrigation for cerumen removal. History of perforation is also an absolute contraindication unless personal knowledge derived from prior examination indicates an intact drum.
Presentation
Perforation symptoms may include audible whistling sounds during sneezing and nose blowing, decreased hearing, and a tendency to infection during colds and when water enters the ear canal. Copious purulent drainage, which may be sanguineous in both acute and chronic perforation, confirms both perforation and infection. Ear canal infections also can cause purulent drainage, but usually in lesser amounts. Perforations uncomplicated by infection or cholesteatoma are never painful. Presence of pain should alert the physician to a concurrent disease process. Perforations accompanied by otorrhea or cholesteatoma are usually not painful.
Indications
Many persons live their lives with tympanic membrane perforations that are entirely without symptoms. Repair of such lesions is usually not indicated. Perforations may be associated with recurrent infection when exposed to water. In swimmers, divers, and other water sports enthusiasts, repair may be indicated as a quality-of-life issue. Hearing loss may be present, especially with larger perforations, and may be a reason for repair. Because a risk to residual hearing exists with every operation on the ear drum, a risk-benefit analysis in which the patient participates is mandatory. For example, question whether the person may be helped just as much with use of a hearing aid.
Relevant Anatomy
The tympanic membrane has 2 distinct zones. The larger of the 2 zones is the pars tensa. This zone consists of a tough and resilient fibrous layer with a diaphanous mucosal layer inside and squamous epithelium outside. The smaller zone is the pars flaccida, which lies superior to the suspensory ligaments of the malleus and lacks a fibrous layer. Perforations of this area often are described as more frequently associated with complications. This is true if the definition of TMP includes depressions of the drum into the middle ear, forming saclike structures (retraction pockets). Clearly, such pockets are more often associated with cholesteatoma formation.
Behind (or medial to) the drum is the middle ear. In front of the drum (or lateral or exterior) is the ear canal. The drum lies at an angle to the bore of the ear canal, creating a vestibule, which can retain cerumen or debris. The malleus is invested by the fibrous layer of the tympanic membrane, securely incorporating it within the drum.
Contraindications
Tympanic membrane perforation (TMP) may be unilateral or bilateral. Select the worse-hearing ear first when performing bilateral tympanic membrane perforation (TMP) repair. If increased hearing loss complications ensue, the better-hearing ear remains uninjured. For the same reason, if tympanic membrane perforation (TMP) is present in a patient's single hearing-capable ear, only incipient life-threatening complications justify repair attempts.

Không có nhận xét nào:
Đăng nhận xét