Introduction
Fractures of the mandibular body may be classified by anatomic location, condition, and position of teeth relative to the fracture, favorableness, or type.
Angle fractures occur in a triangular region between the anterior border of the masseter and the posterosuperior insertion of the masseter. These fractures are distal to the third molar.
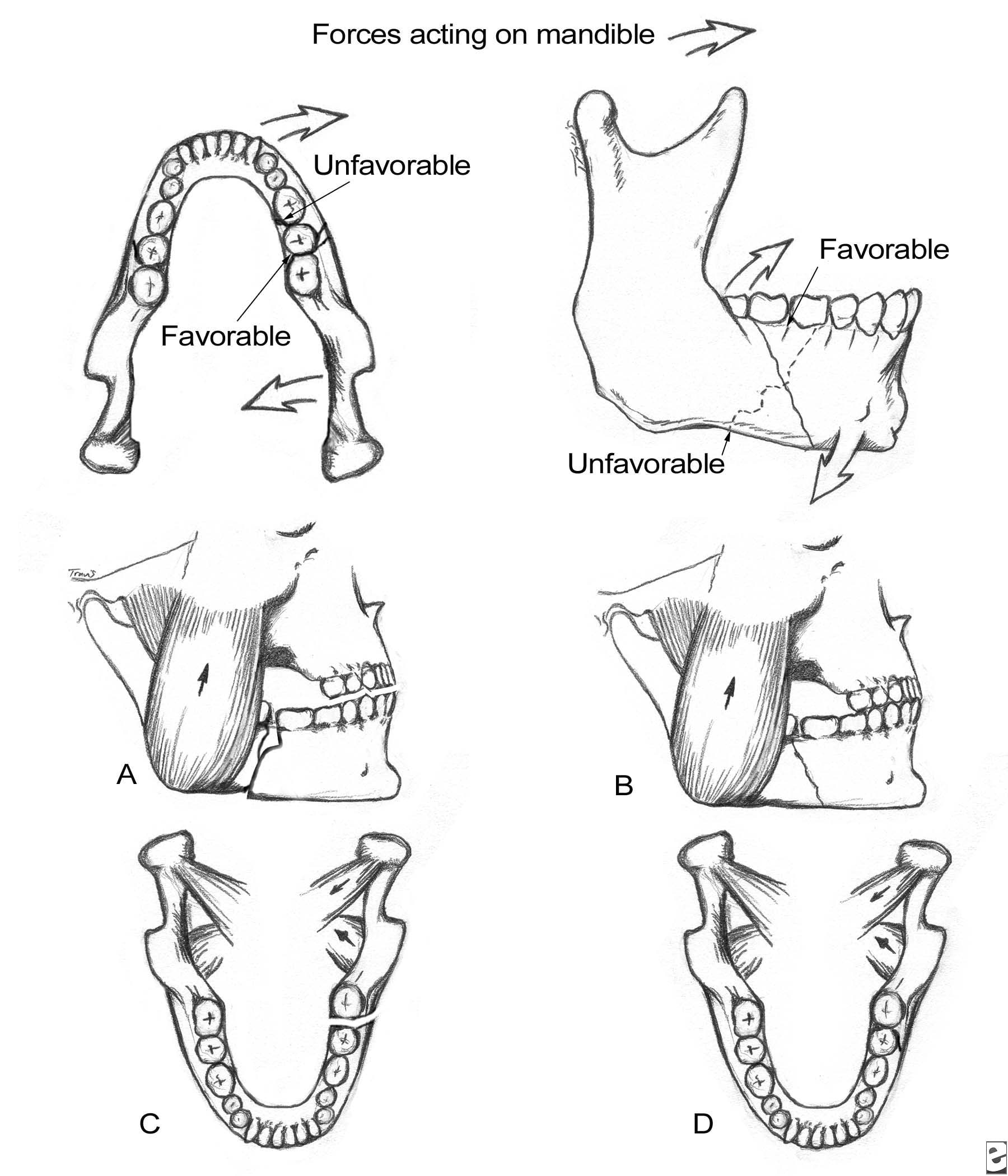
Mandible fractures are also described by the relationship between the direction of the fracture line and the effect of muscle distraction on fracture fragments. Mandible fractures are favorable when muscles tend to draw bony fragments together and unfavorable when bony fragments are displaced by muscle forces. Vertically unfavorable fractures allow distraction of fracture segments in a horizontal direction. These fractures tend to occur in the body or symphysis-parasymphysis area. Horizontally unfavorable fractures allow displacement of segments in the vertical plane.
Angle fractures are often unfavorable because of the actions of the masseter, temporalis, and medial pterygoid muscles, which distract the proximal segment superomedially.
The image below depicts the vertical and horizontal forces acting on the mandible, as well as the relationship of muscle pull to fracture angulation.
Forces acting on the mandible and the relationship between muscle pulls and fracture angulation. A: Horizontally unfavorable. B: Horizontally favorable. C: Vertically unfavorable. D: Vertically favorable.

For excellent patient education resources, visit eMedicine's Breaks, Fractures, and Dislocations Center. Also, see eMedicine's patient education article Broken Jaw.
Problem
The angle of the mandible is the triangular region bounded by the anterior border of the masseter muscle to the posterior and superior attachment of the masseter muscle (usually distal to the third molar). This area may become fractured secondary to vehicular accidents, assaults, falls, sporting accidents, and other miscellaneous causes.
Frequency
In general, incidences of fractures of the mandibular body, condyle, and angle are relatively similar, while fractures of the ramus and coronoid process are rare. The literature suggests the following mean frequency percentages based on location:
- Body - 29%
- Condyle - 26%
- Angle - 25%
- Symphysis - 17%
- Ramus - 4%
- Coronoid process - 1%
The mandible is involved in 70% of patients with facial fractures. The number of mandible fractures per patient ranges from 1.5-1.8. Approximately 50% of patients with a mandible fracture have more than 1 fracture.
In a series of 136 patients with angle fractures, 40% had fractures exclusive to the angle, while 60% had multiple fractures that included an angle fracture.
The mandible fracture patterns of a suburban trauma center found that violent crimes such as assault and gunshot wounds accounted for most fractures (50%), while motor vehicle accidents were less likely (29%).
Etiology
Vehicular accidents and assaults are the primary causes of mandibular fractures throughout the world.
Data from industrialized nations suggest that mandible fractures have various causes as follows:
- Vehicular accidents - 43%
- Assaults - 34%
- Work-related causes - 7%
- Falls - 7%
- Sporting accidents - 4%
- Miscellaneous causes - 5%
Assault most often causes mandible angle fractures.
Pathophysiology
Optimal mandible function requires maintenance of normal anatomic shape and stiffness (ie, resistance to deformation under load). Normal occlusion can be defined when the mesiolabial cusp of the maxillary first molar approximates the buccal groove of the mandibular first molar. Fractures result secondary to mechanical overload. Torque results in spiral fractures; avulsion, in transverse fractures; bending, in short oblique fractures; and compression, in impaction and comminution.
Degree of fragmentation depends upon energy transfer as a result of overload. Therefore, wedge and multifragmentary fractures are associated with higher energy release.
An evidence-based study involving 3002 patients with mandibular fractures found that the presence of a lower third molar may double the risk of an angle fracture of the mandible. Another study compared fractures with wisdom teeth to those without and found an increased infectious risk (16.6%) in fractures with wisdom teeth compared with 9.5% risk in fractures without wisdom teeth.
Presentation
History
Obtain a thorough history specific to preexisting systemic bone disease, neoplasia, arthritis, collagen vascular disorders, and temporomandibular joint (TMJ) dysfunction.
Knowledge of the type and direction of the causative traumatic force helps determine the nature of injury. For example, motor vehicle accidents (MVAs) have a larger associated magnitude of force than assaults. As a result, a patient who has experienced an MVA most often sustains multiple, compound, comminuted mandibular fractures, whereas a patient hit by a fist may sustain a single, simple, nondisplaced fracture.
Knowing the direction of force and the object associated with the fracture also assists the clinician in suspecting and diagnosing additional fractures.
Physical examination
Pertinent physical findings are limited to the injury site.
Change in occlusion may be evident on physical examination. Any change is highly suggestive of mandibular fracture. Ask the patient to compare postinjury and preinjury occlusion.
Posttraumatic premature posterior dental contact (anterior open bite) and retrognathic occlusion may result from a mandibular angle fracture. Unilateral open bite deformity is associated with a unilateral angle fracture.
Anesthesia, paresthesia, or dysesthesia of the lower lip may be evident. Most nondisplaced mandible fractures are not associated with changes in lower lip sensation; however, displaced fractures distal to the mandibular foramen (in the distribution of the inferior alveolar nerve) may exhibit these findings.
Change in facial contour or loss of external mandibular form may indicate mandibular fracture. An angle fracture may cause the lateral aspect of the face to appear flattened. Loss of the mandibular angle on palpation may be because of an unfavorable angle fracture in which the proximal segment rotates superiorly. The anterior face may be displaced forward, causing elongation.
Lacerations, hematoma, and ecchymosis may be associated with mandibular fractures. Their presence should alert the clinician that thorough investigation is necessary to exclude fracture. Do not close facial lacerations before treating underlying fractures except in the case of life-threatening hemorrhage.
Pain, swelling, redness, and localized calor are signs of inflammation evident in primary trauma.
Indications
Use the simplest means possible to reduce and fixate a mandibular fracture. Because open reduction can carry an increased morbidity risk, use closed techniques for the following conditions:
- Nondisplaced favorable fractures
- Grossly comminuted fractures
- Edentulous fractures (using a mandibular prosthesis)
- Fractures in children with developing dentition
- Coronoid and condylar fractures
Indications for open reduction include the following:
- Displaced unfavorable angle, body, or parasymphyseal fractures
- Multiple facial fractures
- Bilateral displaced condylar fractures
- Fractures of an edentulous mandible (with severe displacement of fracture fragments in an effort to reestablish mandible continuity)
Relevant Anatomy
The angle of the mandible is the triangular region bounded by the anterior border of the masseter muscle to the posterior and superior attachment of the masseter muscle (usually distal to the third molar).
Contraindications
Evaluate and monitor the patient's general physical condition prior to treating mandibular fractures.
Any force capable of causing a mandibular fracture may also injure other organ systems. Case reports have documented concurrent posttraumatic thrombotic occlusion of the internal carotid artery and basilar skull fractures.
Bilateral cervical subcutaneous emphysema, pneumothorax, pneumomediastinum, and spleen lacerations have also been associated with mandible fractures after trauma.
Patients should not undergo surgical reduction of mandible fractures until these issues are addressed.

Hi OMFS! This is great overview. I really like your diagram of the muscle pull on the fractures. Did you draw it yourself? Thanks!
Trả lờiXóaI was diagnose with genital warts since 2012 i have be taking lot treatment and all i got is outbreak. in 2015 I gave up the treatment because I can't continues wasting time and money on treatment at the end it will not cure me. about 6 weeks ago i did natural research online I had So many people talking good about natural remedy, after the research i was recommended to Dr onokun, And I wrote to him through his email and told him my problem after some conversations with him he gave me natural treatment after 1 week Dr onokun treated me i got cured permanently. and i went to see my doc he confirmed that the diseases has gone out from my body. every patients should know there is 100% natural hpv cure. contact Dr onokun his email address: dronokunherbalcure@gmail.com
Trả lờiXóa